

Here’s how this started. I kept seeing VIP and KPV mentioned in the same sentence, on the same seller sites, usually with the same vague promise: “anti-inflammatory peptide.” The way they were talked about, you’d think they were two flavors of the same candy bar, pick whichever one your gut (or your fatigue, or your fog) is asking for today. So I did what I always do when something sounds too tidy. I went and read the actual research papers behind both. What I found wasn’t tidy at all, and honestly, that’s the more useful discovery.
Before we get into it: this is an explainer, not medical advice. Both VIP and KPV, when sold for wellness, are compounded products, meaning a pharmacy mixes them to order rather than a factory stamping out an FDA-approved pill. Talk to a licensed clinician before you start either one.
First, what are we even talking about?
Quick vocabulary lesson, because both of these words get thrown around like everybody already knows them. A peptide is just a short chain of amino acids, the building blocks that also make up proteins, only shorter. Think of amino acids as Lego bricks. A protein is a big elaborate castle. A peptide is a small, simple structure, maybe a bridge or a little tower, built from just a handful of those same bricks.
VIP stands for vasoactive intestinal peptide. Don’t let the name fool you into thinking it’s just a gut thing. It’s a 28-amino-acid chain, which in peptide terms is a pretty long structure, and your body already makes it. It behaves less like a simple tool and more like an all-purpose foreman on a construction site: it tells blood vessels to relax, tells glands to secrete, passes messages between nerve cells, and leans on the immune system to calm down when it’s revved up too high. A thorough 2013 review in Amino Acids, written by two researchers who are heavily cited in this specific corner of immunology, Mario Delgado and Doina Ganea, lays out how VIP dials down inflammatory messengers like TNF-alpha while dialing up calming ones like IL-10, nudging the immune system toward tolerance in models of arthritis, colitis, and more (PMID 22139413).
KPV is a completely different kind of object. It’s tiny, just three amino acids: lysine, proline, valine. Those are literally the source of its name (K, P, and V are the shorthand letters for those three). KPV is the tail end of a bigger hormone called alpha-MSH. Here’s the clever part, and it’s genuinely clever: a 2010 review in Advances in Experimental Medicine and Biology explains that this little three-brick fragment is missing the piece alpha-MSH normally needs to lock onto its usual receptor, the docking station cells use to receive its signal. And yet KPV keeps a good chunk of alpha-MSH’s calming effect anyway, apparently by slipping inside the cell and interfering directly with an inflammation switch called NF-kB, sidestepping the receptor altogether (PMID 21222263).
So right out of the gate: one of these is a large, do-everything hormone your body already produces and uses systemically. The other is a stripped-down fragment of a different hormone, doing one narrow job through a back door. They both touch inflammation. That’s about where the similarity ends.
How each one actually does its job
Think of VIP as a hormone with a wide desk. It’s not specialized. It’s got its hand in blood vessel tone, gland secretion, nerve signaling, and immune calming all at once, the way a good general manager touches every department without being an expert plumber or electrician. That breadth is exactly why it’s interesting to researchers, and exactly why it’s hard to pin down and use as a precise drug. When you turn one big dial, a lot of things move.
KPV, by contrast, is more like a tiny key cut for one specific lock. It doesn’t have the parts needed to work the front door (the alpha-MSH receptor), so it found a side entrance into the cell and fiddles directly with one inflammatory switch. That’s a narrower, more surgical kind of action. Narrower doesn’t automatically mean better, it just means the questions researchers ask about it look different.
Where the actual research lives (and why that matters more than the sales pitch)
Here’s the part that reorganized everything in my head, and it’s the part sellers tend to skip past. Forget “which one is more anti-inflammatory” for a second. Ask instead: where, specifically, has each one actually been tested? The two answers turn out to live in almost completely separate rooms.
VIP’s real human testing has happened in the lungs, delivered by inhalation, under medical supervision, in actual diagnosed disease. In a 2003 Journal of Clinical Investigation study, eight patients with primary pulmonary hypertension inhaled VIP and showed improved blood pressure readings in the lungs and better heart output (PMID 12727925). In a 2010 phase II trial in the American Journal of Respiratory and Critical Care Medicine, twenty sarcoidosis patients inhaled nebulized VIP for four weeks safely, with measurable drops in lung TNF-alpha (PMID 20442436). A 2023 review in Life Sciences ties this lung story together and is candid about the catch: VIP breaks down almost instantly once it’s in the body, which makes it genuinely hard to turn into a practical, long-lasting medicine (PMID 37742737).
KPV’s real testing has happened almost entirely in mouse guts and lab dishes. The foundational 2008 paper in Gastroenterology showed KPV hitches a ride into intestinal and immune cells using a transporter called PepT1, and once inside, small amounts quieted inflammatory signaling; oral KPV also reduced the severity of two different chemically induced colitis models in mice (PMID 18061177). A separate 2008 study in Inflammatory Bowel Diseases found KPV calmed inflammation in more mouse colitis models, and it kept working even in mice missing a working melanocortin-1 receptor, backing up that receptor-independent trick. Those same authors said plainly that human trials would be needed before anyone could call this proven (PMID 18092346). Later work, a 2017 Molecular Therapy study, focused on packaging oral KPV into nanoparticles so it could reach the inflamed colon more effectively, again in mice (PMID 28143741).
Put those two paragraphs side by side and the picture clicks into place. VIP has been tested in human lungs. KPV has been tested in mouse intestines. That’s not two products competing for the same customer. That’s two different research programs that happen to share the word “anti-inflammatory.”
The one thing they genuinely have in common, and it’s not good news
Here’s where the skeptic in me got fully justified. Once I lined the two up, the biggest thing they share isn’t a benefit. It’s a gap.
Neither VIP nor KPV has the kind of solid human evidence needed to back the everyday wellness uses they’re actually sold for. I want to be specific here, because “the evidence is limited” gets said so often it’s stopped meaning anything.
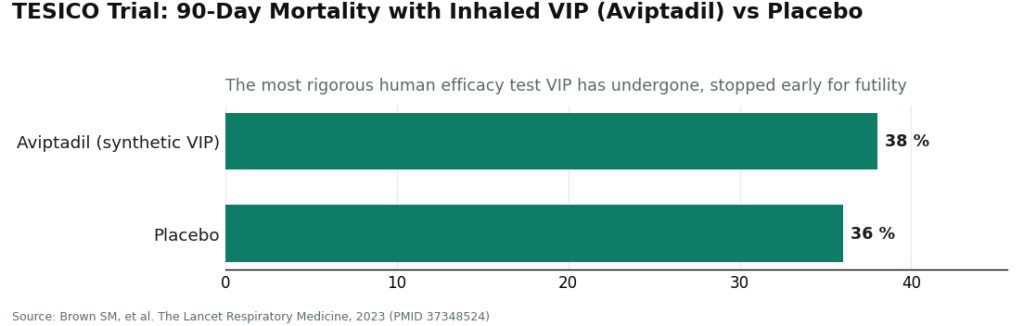
For VIP, wellness sellers push an intranasal spray for fatigue, brain fog, sleep, and a mold-illness condition called CIRS. None of that rests on a large, controlled human trial. And here’s the kicker: the one time VIP got the full rigorous test, an IV version called aviptadil in the TESICO trial during COVID-19, published in The Lancet Respiratory Medicine in 2023 with more than 460 patients, it simply didn’t work. The trial was stopped early for futility. Ninety-day mortality was essentially the same in both groups: 38 percent with aviptadil versus 36 percent with placebo (PMID 37348524). That’s the single most rigorous efficacy data VIP has ever produced, and the answer it gave was no.
For KPV, the gap is arguably wider. I couldn’t find a single adequately sized, randomized, controlled human trial showing KPV treats any condition in actual people. Every promising result comes from cells in a dish or animals in a cage. The mechanism is real, the mouse-gut data is genuinely interesting to read, but the human proof isn’t thin. It’s basically not there, and the researchers themselves said so back in 2008 (PMID 18092346).
So the honest shared trait is this: two legitimate molecules with real, documented biology, and real early-stage or animal signals, both being sold for everyday human problems that no solid human trial has actually tested. That sentence never makes it onto a product page, and it’s the single most important thing to know before you spend money on either.
So which one fits your goal? A straight attempt at an answer
You want a “just tell me which one” answer, so here’s my honest attempt, with a big flashing caveat: I’m matching molecules to where their research actually points, not promising results.
If your interest is lungs or whole-body inflammation, VIP is the one with human data behind it, thin as that data is. Notice the catch, though: that human data used inhaled VIP, under a doctor’s care, in people with diagnosed lung disease. That’s a very different thing from a nasal spray shipped to your house for fatigue. So even here, the honest match is “VIP is where the human evidence lives,” not “VIP will fix your inflammation.”
If your interest is gut inflammation, KPV is the molecule whose research is actually aimed there, but every bit of it is preclinical, meaning it hasn’t gotten past animals and lab dishes into human trials. The mechanism is promising on paper and unproven in people.
If your goal is vague, general “anti-inflammatory wellness,” neither peptide has earned your trust, and that’s the honest answer, not a cop-out. Most people asking “which one should I take” actually have this vague goal, and it’s the one the evidence supports least for either molecule. Choosing between VIP and KPV for general inflammation is choosing between two unproven things. The smarter move is to lower your expectations and raise your scrutiny of wherever you’d buy it from.
I won’t hand you a confident little chart matching each peptide to a symptom, because that would pretend to a precision the research just doesn’t have. The best I can offer is this: let your goal point you toward whichever molecule’s research at least aims in that direction, while keeping firmly in mind that “aims at it in a mouse” and “proven in you” are nowhere near the same thing.
What matters more than picking the “right” peptide
Here’s the part that actually surprised me by the end of all this reading. Once you accept that both molecules are unproven for the reasons people buy them, the choice between VIP and KPV stops being the most important decision on the table.
Think about what you actually control here. If neither peptide is proven, then what protects you isn’t which one you pick, it’s whether a real clinician is involved, whether a licensed pharmacy made the product so you actually know what’s in the vial and at what strength, and whether whoever sold it to you was straight with you about how thin the evidence is. Those three things matter identically whether you’re holding VIP or KPV. Get any of them wrong and the molecule you chose stops mattering, because now you’re taking an unverified, unsupervised compound either way.
That’s the whole reason a supervised, compounded-pharmacy model matters here, and it matters the same for both peptides. FormBlends is one provider that offers VIP and KPV set up that way: a licensed clinician involved in the decision, a licensed US compounding pharmacy actually making the product, and the not-FDA-approved, compounded status stated up front instead of buried in fine print. I’m naming it as an example of the setup worth looking for, not as a scoreboard pick over anyone else, because the setup is the actual point. Clinician. Licensed pharmacy. Honest labeling. Whichever peptide you’re leaning toward, hold whoever sells it to that same bar, because when both compounds are uncertain, the source is the one variable you can actually check.
Quick answers to what people actually ask
Are VIP and KPV basically the same thing? No. VIP is a large, 28-amino-acid hormone your body makes, studied mainly in human lungs. KPV is a three-amino-acid fragment of a different hormone, studied mostly in mouse guts. Both touch inflammation, but they’re different tools with evidence sitting in completely different places.
Which one is better for inflammation? Depends what kind, and neither is proven in people. VIP has small human lung data. KPV has preclinical gut data. For general, vague anti-inflammatory wellness, neither has solid human backing, and that’s the honest answer.
Does either one have real human trials behind how it’s marketed? Not for the everyday uses they’re sold for. VIP’s one large, rigorous trial (TESICO) came back negative. KPV has essentially no adequately sized human efficacy trials at all. Both are biologically real and clinically unproven for those specific claims.
If I have to choose just one, how do I decide? Match it to where its research actually points: lungs or whole-body inflammation leans VIP, gut inflammation leans KPV. Then remember “shown in animals” isn’t “shown in you,” keep expectations modest, and spend most of your energy vetting who you’d get it from.
What matters more than the choice between them? The source. Since both are unproven, having a licensed clinician and a licensed pharmacy behind the product matters more than which peptide you land on. That’s the part you can actually verify, and it’s the same requirement for both.
Bottom line
I went in thinking I’d referee a contest between two similar peptides. I came out realizing the contest was mostly a marketing illusion. VIP and KPV are different molecules, tested in different organs, in different species, at different stages of research, and the thing they most genuinely share is that neither has earned the everyday wellness claims stapled to it. If your interest is lungs or systemic inflammation, VIP is where the human data, thin as it is, actually sits. If your interest is gut inflammation, KPV is where the research points, entirely in animals so far. But for most people asking “which one,” the better question is “from whom,” because with two uncertain compounds, a real clinician, a licensed pharmacy, and honesty about how thin the evidence is will protect you far more than getting the peptide “right” ever will. Not the conclusion I expected to land on. It’s the one the reading actually supports.
VIP and KPV are compounded, prescription-style products that are not FDA-approved. Talk with a licensed healthcare provider before starting or changing anything you take.
Verified primary sources
These PMIDs were checked directly on PubMed; each resolves to the paper described and supports the specific claim attached to it. The VIP sources are reused from the verified VIP hub set; the KPV sources are reused from the verified KPV hub set.
VIP:
- Delgado M, Ganea D. Vasoactive intestinal peptide: a neuropeptide with pleiotropic immune functions. Amino Acids. 2013. PMID 22139413. https://pubmed.ncbi.nlm.nih.gov/22139413/ . Review of VIP’s anti-inflammatory and immune-regulatory biology.
- Petkov V, Mosgoeller W, Ziesche R, et al. Vasoactive intestinal peptide as a new drug for treatment of primary pulmonary hypertension. Journal of Clinical Investigation. 2003. PMID 12727925. https://pubmed.ncbi.nlm.nih.gov/12727925/ . Eight-patient inhaled-VIP study.
- Prasse A, Zissel G, Lützen N, et al. Inhaled vasoactive intestinal peptide exerts immunoregulatory effects in sarcoidosis. American Journal of Respiratory and Critical Care Medicine. 2010. PMID 20442436. . Phase II nebulized-VIP trial in 20 sarcoidosis patients.
- Brown SM, Barkauskas CE, Grund B, et al. Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial. The Lancet Respiratory Medicine. 2023. PMID 37348524. . Large negative RCT of synthetic VIP (aviptadil).
- Zhong HL, Li PZ, Li D, et al. The role of vasoactive intestinal peptide in pulmonary diseases. Life Sciences. 2023. PMID 37742737. . Review including VIP’s rapid degradation and stalled development.
KPV:
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HTT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008. PMID 18061177. . KPV enters cells via PepT1 and reduced DSS- and TNBS-induced colitis in mice.
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflammatory Bowel Diseases. 2008. PMID 18092346. . KPV eased mouse colitis and worked in MC1R-deficient mice; authors note human trials are still needed.
- Xiao B, Xu Z, Viennois E, et al. Orally targeted delivery of tripeptide KPV via hyaluronic acid-functionalized nanoparticles efficiently alleviates ulcerative colitis. Molecular Therapy. 2017. PMID 28143741. . Oral KPV nanoparticles reduced DSS-induced colitis in mice.
- Brzoska T, Böhm M, Lügering A, et al. Terminal signal: anti-inflammatory effects of alpha-melanocyte-stimulating hormone related peptides beyond the pharmacophore. Advances in Experimental Medicine and Biology. 2010. PMID 21222263. . Review explaining the KPV fragment’s receptor-independent anti-inflammatory activity.
On compounded-drug regulatory status, see the FDA’s overview of human drug compounding:
What exactly is VIP peptide, in plain terms?
VIP, short for vasoactive intestinal peptide, is a 28-amino-acid chain your body already builds on its own. It shows up in the gut, the lungs, and the nervous system, where it helps relax muscle, regulate immune signaling, and even keep your circadian rhythm on schedule. The synthetic version sold online is meant to copy that natural molecule, but copying something your body makes in tiny, tightly controlled amounts is a lot harder to pull off well than most sellers admit.
Is it actually legal to buy VIP peptide in the US right now?
Honestly, it’s murky. VIP isn’t an FDA-approved drug you can just buy off a shelf, and the agency has been cracking down on peptides marketed as “research chemicals” or supplements. A licensed compounding pharmacy can legally prepare it for a specific patient under a prescriber’s order. Ordering it from a random website almost certainly lands you in a gray zone, if not an outright illegal one. The rules shifted meaningfully in 2023 and are still moving, so check current FDA guidance rather than assuming last year’s answer still holds.
What side effects show up with VIP peptide?
In clinical research settings, the effects reported most often are flushing, low blood pressure, nausea, and headache, all of which line up with VIP’s job of relaxing blood vessels. Some people also report fatigue or dizziness shortly after dosing. Because most people buying it online are dosing themselves without medical supervision and with no verified purity on what’s actually in the vial, the real-world side effect picture is probably wider than what the small clinical studies caught. That gap is worth taking seriously.
Does the research really back using VIP for CIRS or mold illness?
There’s some early, physician-led work suggesting VIP might help certain patients with Chronic Inflammatory Response Syndrome, mostly coming out of mold-illness clinics. But those studies are small, haven’t been independently repeated at any real scale, and used pharmaceutical-grade material under close medical supervision, not peptides ordered off a website. If you’re genuinely considering this path, a physician-supervised compounding pharmacy such as FormBlends is the accountable route, not a supplement storefront.


